by Brian T. Lynch, MSW
 Forget the Swedish or the German model for controlling the COVID-19 pandemic. The United States should develop its own alternative model to control the outbreak, one based on science and the particular demographic data that have emerged about this disease.
Forget the Swedish or the German model for controlling the COVID-19 pandemic. The United States should develop its own alternative model to control the outbreak, one based on science and the particular demographic data that have emerged about this disease.
An alternative approach is urgently needed because, a) a general lockdown of the entire country and its economy cannot be sustained for long, and b) the more obstreperous elements of our population, and the billionaire elites who may be pulling their strings, are already forcing states into lifting restrictions on everyone. We are heading into what will likely be a disastrously premature reopening of the economy
America is trapped in a binary choice between letting COVID-19 run its natural course or locking down society to minimize the infections and deaths until a vaccine is available. The ultimate civilized goal in a pandemic is to achieve herd immunity through vaccinations, or by any other scientific means that results in the least possible loss of life. In the absence of any civil interventions, a novel virus simply runs rampant through the population at exponential speed, making almost everyone sick and killing millions if it is a lethal strain. In the absence of vaccinations, people who recover from the novel virus are likely to develop antibodies that will prevent reinfection for some period of time, although there are exceptions. When enough people in a population have immunity following their illness or through inoculations, the whole population develops herd immunity. This means that even those people who are susceptible to illness when exposed to the virus are rarely ever exposed to it. They are safely buffered by the many people around them who are immune.
There are two demographic characteristics of COVID-19 morbidity and mortality rates that appear significant and potentially useful in creating an alternative approach to controlling the pandemic. The first is the very differential mortality rates according to age, and the second is emerging evidence that up to 50% of individuals who contract the virus never display any symptoms of the illness. Look at the mortality differentials first.
HIGH-RISK GROUP
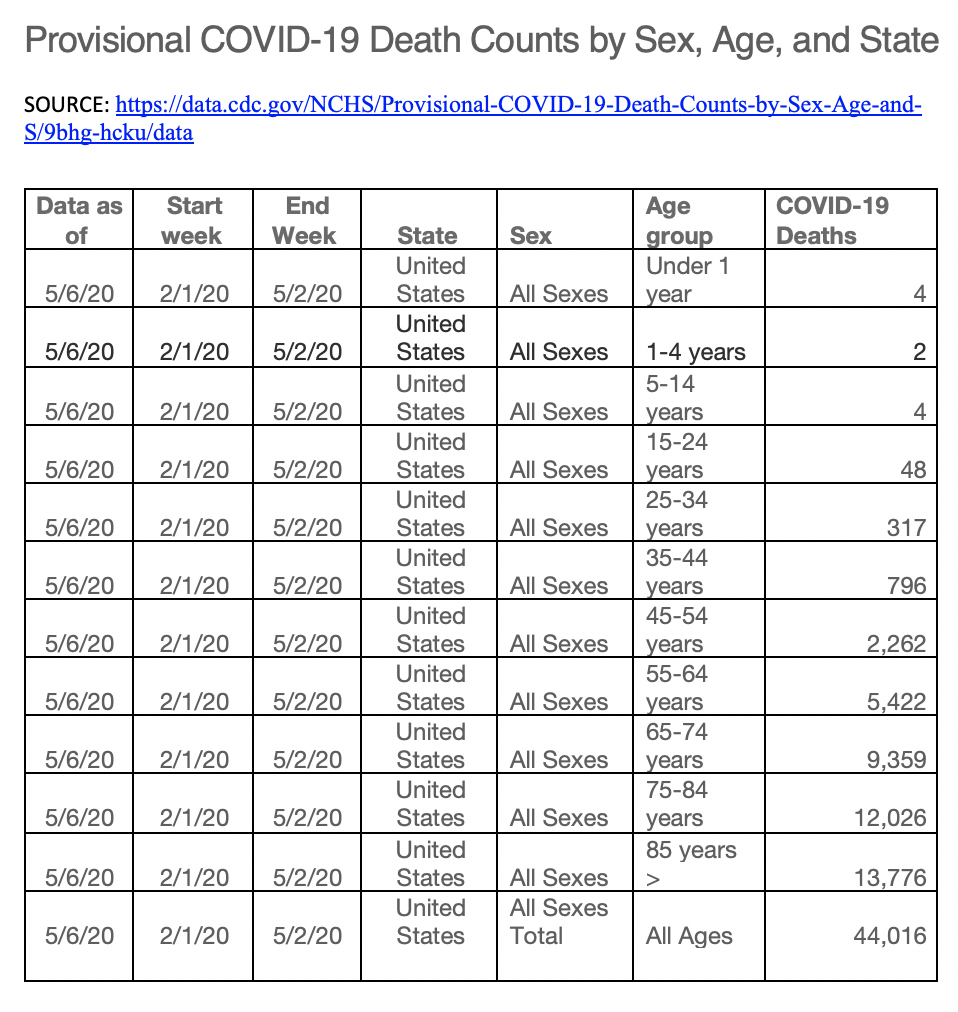
CDC data (see table below) shows that 97% of COVID-19 deaths are of people 45-years-old or older. This agrees with data collected in Sweden, China, and other countries. Also, death rates are much higher in people with underlying health conditions. From these data we know that there is a high-risk group that requires optimal protection from exposure to COVID-19. It follows that any adults caring for people in this high-risk group also need to be optimally protected from exposure to the virus. High-risk individuals by age or underlying medical conditions and their caregivers should be allowed to remain in social lockdown in those states that are starting to life restrictions.

When the data in this CDC age/mortality rate table are pictured in a bar graph, the trendline reveals an exponentially rising mortality rate with age. It turns out that 97% of all COVID-19 deaths are of people over the age of forty-five.


Given how many nursing home and congregate care facility residents are getting sick and dying in the United States it would be tempting to believe that poor medical care in these facilities accounts for the high mortality rates, and this might skew the demographics on age and mortality in the data. There is an unacceptably high number of residents getting infected in these facilities, and this is on the corporations that run these facilities. But the high mortality rate of the infected residents may not be due to inferior care so much as the correlation between age and mortality of the disease. The publically available global data on age and mortality shows the same exponential rise in mortality with advancing age in South Korea, Spain, China, and Italy. (see below)

An alternative approach is urgently needed because, a) a general lockdown of the entire country and its economy cannot be sustained for long, and b) the more obstreperous elements of our population, and the billionaire elites who may be pulling their strings, are already forcing states into lifting restrictions on everyone. We are heading into what will likely be a disastrously premature reopening of the economy
America is trapped in a binary choice between letting COVID-19 run its natural course or locking down society to minimize the infections and deaths until a vaccine is available. The ultimate civilized goal in a pandemic is to achieve herd immunity through vaccinations, or by any other scientific means that results in the least possible loss of life. In the absence of any civil interventions, a novel virus simply runs rampant through the population at exponential speed, making almost everyone sick and killing millions if it is a lethal strain. In the absence of vaccinations, people who recover from the novel virus are likely to develop antibodies that will prevent reinfection for some period of time, although there are exceptions. When enough people in a population have immunity following their illness or through inoculations, the whole population develops herd immunity. This means that even those people who are susceptible to illness when exposed to the virus are rarely ever exposed to it. They are safely buffered by the many people around them who are immune.
There are two demographic characteristics of COVID-19 morbidity and mortality rates that appear significant and potentially useful in creating an alternative approach to controlling the pandemic. The first is the very differential mortality rates according to age, and the second is emerging evidence that up to 50% of individuals who contract the virus never display any symptoms of the illness. Look at the mortality differentials first.
HIGH-RISK GROUP
CDC data (see table below) shows that 97% of COVID-19 deaths are of people 45-years-old or older. This agrees with data collected in Sweden, China, and other countries. Also, death rates are much higher in people with underlying health conditions. From these data we know that there is a high-risk group that requires optimal protection from exposure to COVID-19. It follows that any adults caring for people in this high-risk group also need to be optimally protected from exposure to the virus. High-risk individuals by age or underlying medical conditions and their caregivers should be allowed to remain in social lockdown in those states that are starting to life restrictions.

A confirming set of data that looks at age and hospitalization rates produces a similar pattern (see below). This graph was produced by the CDC. And it does make sense that those who are more deathly ill would be more likely to require hospitalization. Taken together it makes sense that limiting exposure to this age-related high-risk group should lower both mortality rates and hospitalization rates, thus helping to prevent our health care system from becoming overwhelmed.


NON-PERSONAL-RISK GROUP
There is data that suggests as many as 50% of the population may carry the COVID-19 virus while remaining symptom-free. These people apparently test positive for the active virus but remain free of illness. During the period of their contagion, however, they remain a vector for exposing others to COVID-19. This makes them especially dangerous to others while they, and others like them, are not at risk of illness or death themselves. Furthermore, if the bodies of symptom-free individuals ultimately eliminate the virus, these people may also develop antibodies to prevent another contraction of the virus. If their bodies have some other way of fighting COVID-19, that should be studied investigated as it might lead to effective new therapies.
A careful analysis of the characteristics of this non-personal risk group should be conducted at once to sees if researchers can reliably identify who is likely to be asymptomatic after exposure to COVID-19. If people in this category can be reliably identified, then at the least these would people for whom initial phases of vaccinations efforts would not be as critical. That would greatly focus resources while manufacturing of the eventual vaccine is scaling up.
MODERATE-RISK GROUP
If identifying individuals who are at not at personal risk of coronavirus illness can be accomplished without any special testing (say on a demographic basis) then identifying them would be advantageous for a number of other reasons. One advantage would be to create a middle group of people who fall outside of both the high-risk category and non-personal-risk group. This middle group of people would likely mildly to moderate symptoms when exposed to COVID-19. This group of people would know that have to maintain appropriate safety precautions to prevent getting sick when they become exposed to the virus. The greater certainty of having this knowledge would help inform their decisions and behavior when reintegrating back into a less regulated environment as states begin opening up the economy. These are also the people who would most benefit from testing, isolation, and contact tracing to control the spread of the virus. Being a smaller subset of the population, this would help target precious testing capacity and focus it where it would do the most good. When members of this group do recover from the illness, they will presumably have developed immunity that can allow them the non-personal-risk group.
There is data that suggests as many as 50% of the population may carry the COVID-19 virus while remaining symptom-free. These people apparently test positive for the active virus but remain free of illness. During the period of their contagion, however, they remain a vector for exposing others to COVID-19. This makes them especially dangerous to others while they, and others like them, are not at risk of illness or death themselves. Furthermore, if the bodies of symptom-free individuals ultimately eliminate the virus, these people may also develop antibodies to prevent another contraction of the virus. If their bodies have some other way of fighting COVID-19, that should be studied investigated as it might lead to effective new therapies.
A careful analysis of the characteristics of this non-personal risk group should be conducted at once to sees if researchers can reliably identify who is likely to be asymptomatic after exposure to COVID-19. If people in this category can be reliably identified, then at the least these would people for whom initial phases of vaccinations efforts would not be as critical. That would greatly focus resources while manufacturing of the eventual vaccine is scaling up.
MODERATE-RISK GROUP
If identifying individuals who are at not at personal risk of coronavirus illness can be accomplished without any special testing (say on a demographic basis) then identifying them would be advantageous for a number of other reasons. One advantage would be to create a middle group of people who fall outside of both the high-risk category and non-personal-risk group. This middle group of people would likely mildly to moderate symptoms when exposed to COVID-19. This group of people would know that have to maintain appropriate safety precautions to prevent getting sick when they become exposed to the virus. The greater certainty of having this knowledge would help inform their decisions and behavior when reintegrating back into a less regulated environment as states begin opening up the economy. These are also the people who would most benefit from testing, isolation, and contact tracing to control the spread of the virus. Being a smaller subset of the population, this would help target precious testing capacity and focus it where it would do the most good. When members of this group do recover from the illness, they will presumably have developed immunity that can allow them the non-personal-risk group.
Reopening the economy will require a transition from our current Lockdown status to a Testing, Isolating, and Contact Tracing (TICT) strategy focused initially on adults re-entering the workforce from the moderate risk and no-personal risk groups. The availability of COVID-19 testing has to be significantly increased by perhaps a factor of 10 times the current rate nationally. Until a vaccine or effective treatment is available, TICT efforts remain the best hope for controlling infection rates. This three-tiered method of controlling the virus would permit a safer means to gradually reopen the economy and relieve the economic burdens on us all. It would allow us to direct medical and economic resources to where they are most needed and most necessary. When a vaccine is finally developed, this approach would pre-identify those who need to be inoculated first, thus not wasting precious doses on those for whom it is not in immediate need.
Pie in the sky? Maybe, but it is worth consideration.

No comments:
Post a Comment
Please feel free to comment or make suggestions